Background
Milliman completed a study of how the transition from Risk Adjustment Processing System (RAPS) data to Encounter Data System (EDS) data is affecting the payment year (PY) 2016 risk scores and revenue for Medicare Advantage (MA), also known as Medicare Part C. Fifteen Medicare Advantage organizations (MAOs) participated in the study, reflecting a cross-section of small and medium size organizations and representing over 900,000 members in 154 plans. The study relied on the revised EDS MAO-004 files that the Centers for Medicare and Medicaid Services (CMS) released late in October 2016. This article is the second in a series of articles on the transition to EDS. Read the first paper for more details about the EDS and RAPS data used in MA risk scores.
Overview of study results
Overall, the study found that the median percentage difference between PY 2016 risk scores based on RAPS and the EDS-based risk scores is 4.0%. The percentage difference is larger for special needs plans (SNPs) and smaller for general enrollment plans as shown in Figure 1. The prior year’s diagnoses make up a larger component of SNP members’ risk scores, compared to general enrollment plans, so the risk score impact for SNP plans is larger.
Figure 1: Part C risk score difference percentiles (EDS vs. RAPS)
| Plan type | 20th | 40th | 50th | 60th | 80th |
| All plans | -7.2% | -4.8% | -4.0% | -3.4% | -2.6% |
| SNPs | -8.4% | -6.6% | -5.1% | -4.7% | -3.1% |
| General enrollment | -6.8% | -4.2% | -3.8% | -3.2% | -2.5% |
|
Note: Members included are non-end-stage renal disease (ESRD)/non-hospice members who were enrolled during the entire calendar year 2015. |
|||||
We have not attempted to quantify what portion of the difference between RAPS and EDS is due to incompleteness of the EDS submissions, issues with CMS’s return files (revised MAO-004 files), changes to filtering logic, and the effect of claims coding errors.
As an illustration, the potential Part C PY 2016 revenue using the median difference of -4% between RAPS and EDS results in a reduction of approximately $40 per member per year, assuming approximately $800 in Part C risk-adjusted revenue and a 1.0 RAPS-only risk score. To the extent that this -4% gap persists in future years, the revenue impact will grow because the EDS-based risk score will make up an increasing portion of the final risk score (e.g., with the 25% EDS weight in PY 2017, the per member reduction would be about $100 per year).
Member-level differences
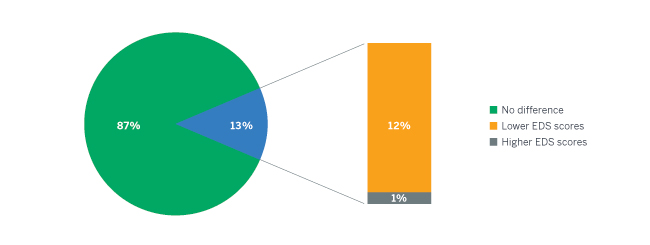
Figure 2 presents the distribution of differences between the Part C RAPS and EDS risk scores, showing that 87% of the members in the study had the same Part C risk score under RAPS and EDS, 12% of members had lower EDS risk scores, and 1% had higher EDS risk scores. The distribution is based on the estimated final PY 2016 risk scores for members enrolled in 2015. We saw more differences in the Medicare Part D risk score than in the Part C risk scores—only 80% of the Part D risk scores were the same. Additionally, about 1% of Part C members’ EDS risk scores were a full unit (1.0 risk score unit) lower than their RAPS risk scores.
Figure 2: Member-level comparison of EDS and RAPS Part C risk scores
New CMS information on EDS risk scores
Since our last paper on the topic, CMS has released a new memo regarding risk adjustment data deadlines. The December 29, 2016, memo1 from CMS announced two changes to the data submission and risk score calculation schedules that were previously released:
- Submission deadline for EDS data has been extended for the 2016 final risk scores: The final day to submit encounter data for use in PY 2016 risk scores has been extended to May 1, 2017 (updating the original deadline of January 31, 2017). The RAPS submission deadline was not extended and remains January 31, 2017. It is our understanding that there have been a few instances where the MAO-004 reports from CMS were unintentionally missing diagnosis data because of internal CMS errors, and so this extension gives MAOs additional time to react as CMS makes fixes available.
- 2017 mid-year risk score updates will be based only on RAPS: As a departure from original plans, CMS will not calculate the 2017 mid-year risk scores using EDS, RAPS, and Medicare fee-for-service (FFS) claims. Initially, the 2017 PY was going to be the first year where the mid-year risk scores would show the blended EDS/RAPS risk scores (using the 25%/75% weights for 2017). MAOs will have to wait until final risk score reconciliation in August 2018 in order to know the true effect of EDS data on their PY 2017 risk scores and revenue. Therefore, PY 2017 will not be much different from PY 2016 with respect to any early information on the EDS data impact. The deadline for submitting EDS and RAPS data for mid-year risk score calculation is unchanged from March 3, 2017.
MAOs have more time to review their EDS diagnosis submissions between now and May 1, 2017, in order to improve any deficiencies in their EDS submission processes. As we outlined in our first paper, MAOs should consider the following steps on their diagnosis submissions:
1) Calculate risk scores from each source: EDS return files (MAO-004s), RAPS return files, and detailed source data.
2) Compare risk scores resulting from each source.
3) Identify submission gaps and coding gaps, and quantify the effect.
4) Prioritize and resolve process gaps.
The delay in providing early information to MAOs on PY 2017 risk scores also underscores the necessity of MAOs performing their own calculations of risk scores from the two sources in order to monitor earned revenue and identify any diagnosis submission issues.
Ongoing transition problems
Working with the survey participants and other MAOs shed light on several problems which MAOs are still struggling with:
- Implementing a successful EDS submission process: There were several MAOs that were interested in participating in the study, but they had insufficient EDS return file data available at the time. Examples include delays that are due to internal EDS implementation or to problems with source data capture. Conversely, there were several MAOs that believed they had a strong EDS submission process in place and, therefore, felt they would not benefit from participating in the study.
- Difficulty in submitting chart review data through EDS: MAOs have reported difficulties getting linked and unlinked chart review records accepted under EDS. For the MAOs we helped to identify the root cause of EDS and RAPS risk score differences, the rejection of chart review data was a common problem. There is also concern that unlinked chart review data may not be accepted by CMS in the future.
- Lack of reliable MAO-004 data prior to October 22, 2016: The submission deadline for calendar year 2015 diagnosis codes that will affect PY 2016 revenue is January 31, 2017, for RAPS submissions, and May 1, 2017, for EDS submissions. Given the delays releasing corrected MAO-004 return files, a limited amount of time is available for MAOs to identify and correct diagnosis submission problems. On top of the multiple revisions to the MAO-004 files, it has been a challenge for MAOs to know the effect of the RAPS to EDS transition because CMS has not provided feedback on the impact of EDS data on risk scores and revenue (e.g., by including the EDS effect in the mid-year update to PY 2016 risk scores and revenue). The current monthly membership report (MMR) risk scores and revenue reflect only RAPS and FFS submissions. MAOs will not know the full impact of EDS submissions on PY 2016 revenue until after the May 1, 2017, submission deadline. This same challenge will persist for PY 2017 risk scores as we described above.
- The utility of MAO-002 reports: There are currently no diagnosis data in the MAO-002 encounter data processing status reports, making it difficult for MAOs to immediately assess the effect of the rejected records under EDS. MAOs must set up a process where EDS submission results are linked back with the source diagnosis data in order to immediately assess the risk score impact of accepted and rejected diagnosis records. Without setting up this linkage, MAOs must wait for the MAO-004 return files from CMS, which have not been released on schedule.
- The effect of new filtering logic: Because the EDS process introduces new filtering logic in addition to a new process for submitting diagnosis data, it is difficult for MAOs to isolate which risk score reductions are driven by submission process issues versus filtering issues. As discussed in our first paper, a comprehensive method for separating the impact of filtering and submission process issues is to independently apply the EDS filters to the MAO's source systems and calculate the expected risk scores by member.
Conclusion
The transition to EDS-based risk scores will have a significant effect on MAOs in PY 2016 and future years. The participants in our study saw a median decrease in risk scores of 4% when comparing EDS scores with RAPS scores. In addition to the reduced risk scores and revenue that are expected to result from this transition, MAOs have been challenged with difficult problems related to EDS data submission and receiving information in a timely manner. Despite revisions from CMS, these issues are not fully resolved. It is important that MAOs implement their own processes of calculating, reviewing, and monitoring their EDS and RAPS risk scores in order to identify problems early and resolve them before submission deadlines in order to avoid unnecessary revenue reductions.